Pediatric Health Technology Incubator Laboratory
Dr. James Wall has the expertise and experience to take medical device concepts from idea to bedside. His specific areas of investigational interest include the design and development process of medical devices as well as the translation of minimally invasive technologies into pediatric surgical practice. He has worked on studies of novel minimally invasive surgical techniques and devices in animal models to minimize risk in translation of technology to human use, and then safely brought these techniques into clinical use. He has additional technology transfer experience including the development of multiple medical devices as an inventor, chief medical officer, consultant and board member.
Mission Statement
To discover and develop health technologies that improve children’s lives
Research Director

James Wall
Dr Wall is an Associate Professor of Paediatric Surgery and Bioengineering, and is the Director of Program Development for the Stanford Biodesign Fellowship Program where he mentors and advices starting entrepreneurs in the medical device space.
Dr Wall was born in London, England and immigrated to the United States at a young age, attending high school in Mobile, Alabama. He went on to attend Tulane University, where he received an undergraduate degree in Biomedical Engineering, graduating Summa Cum Laude. Following college, he was accepted to the University of Pennsylvania’s School of Medicine. During medical school, he co-wrote a business plan that received semi-finalist honors at the Wharton business plan competition. The plan became a start-up company, which he developed through the Wharton Venture Initiation Program. After completing medical school, Dr Wall moved on to a General Surgery residency training program at the University of California, San Francisco. After completion of his residency he attended the Biodesign Innovation fellowship at Stanford and went on to complete a fellowship in minimally invasive surgery at the IRCAD in France and a fellowship in pediatric surgery at Lucile Packard’s Children Hospital.
Dr. Wall began his scientific career investigating less invasive means of performing surgical interventions. As a junior member of a team at the IRCAD institute in France, he was able to perform the laboratory, engineering and animal groundwork of the several medical device contributions. His next focus was on developing his own program to investigate less invasive approaches to pediatric surgical problems. In collaboration with colleagues at UCSF and other institutions he was able to lead to lead a major initiative in understanding the potential application of a magnetic anastomosis device and how that device could be delivered endoscopically to perform intestinal surgery without incisions. This device is currently in development under an Investigation Device Exemption from the FDA and has been safely used in human trials. As a practicing pediatric surgeon, he has contributed as an investigator on multiple clinically studies of minimally invasive pediatric surgical techniques. In the last 3 years, he has in addition begun a clinical program in flexible endoscopic surgery in children. His team safely translated devices and techniques from adult surgery to small children including the first Per-Oral Endoscopic Myotomy performed at Children’s Hospital in the United States in 2013. Finally, he has contributed over the past 10 years as an inventor, founder, chief medical officer and consultant to multiple medical device companies across a breath of medical needs including epidural anesthesia, pediatric surgery, venous stasis and umbilical catheters. He was the inventor, founder, early CEO and ultimately the Chief Medical Officer of InSite Medical Technologies, which was a venture capital backed company that brought a novel epidural anesthesia product to the market. And is currently the assistant director of the Stanford Biodesign program focused on training medical device innovators. Through these experiences, he has learned the skill set to create, develop and commercialize medical devices.
Research Team

Orestis Vardoulis
Orestis grew up in a small Greek town, and for as long as he can remember, he was always fascinated by machines.
This passion led him to study mechanical engineering at the Aristotle University of Thessaloniki, where he focused on fluid mechanics and turbo machinery. For his thesis, Orestis focused on the field of biomedical engineering where he applied fluid flow principles to simulate the function of a glaucoma drainage device. This experience of leveraging his engineering skills to address real clinical problems had an impact on his career focus, and Orestis decided to pursue a PhD in Biotechnology and Bioengineering at the École Polytechnique Fédérale de Lausanne (EPFL) in Switzerland. His thesis titled “Novel non-invasive techniques for hemodynamic monitoring” won the 2014 EPFL Chorafas award. In parallel, Orestis was invited to complete a research internship at Microsoft Research in Redmond, WA, where he contributed to developing a novel wearable device for monitoring cardiovascular health. Shortly after, Orestis joined Advanced Sport Instrument, a Swiss startup specializing in wearable monitoring for sports performance optimization. In early 2016, Orestis received a grant from the Swiss National Science Foundation and joined the lab of Professor Zhenan Bao at Stanford Chemical Engineering where he worked in a variety of projects spanning wearable health monitoring devices and self-healing electronics for wearable and IOT applications. Most recently, Orestis was selected as one of the 2017-2018 Biodesign Innovation Fellows and spent a year learning the Biodesign Innovation process that applies design-thinking principles for medical technology innovation. During his journey, he had the opportunity to work with amazing collaborators and publish multiple research articles and patents in the space of cardiovascular physiology, sensors, nanotechnology, signal processing, and magnetic resonance imaging among other domains. Orestis is particularly excited to leverage his multifaceted skillset to identify and address unmet clinical needs in the pediatric population and to take part in an exciting and interdisciplinary environment such as the Pediatric Health Technology Incubator Laboratory.

Juliana Perl
Juliana's interest in healthcare innovation started as a child standing on a step stool, watching her father perform surgery.
She went on to study Product Design at Stanford where she learned to root all innovation in thoroughly researched user needs and worked alongside nonprofit organizations working to improve healthcare delivery and education in low-resource settings. After graduating, Juliana joined the team at Health Advances, a healthcare strategy consulting firm. She supported healthcare technology companies and investors in their commercial strategy decisions, working to drive the adoption of innovations that improve healthcare. Her projects included medical devices, diagnostics, digital health, and biopharmaceuticals across continents. Juliana is now a master’s student in Management Science and Engineering with a focus on technology entrepreneurship. She is thankful to have the opportunity to learn about device development with Dr. Wall’s team and to focus on the meaningful space of pediatric health.
Research Projects
Endoflip
Pediatric Endoluminal Functional Lumen-Imaging Probe
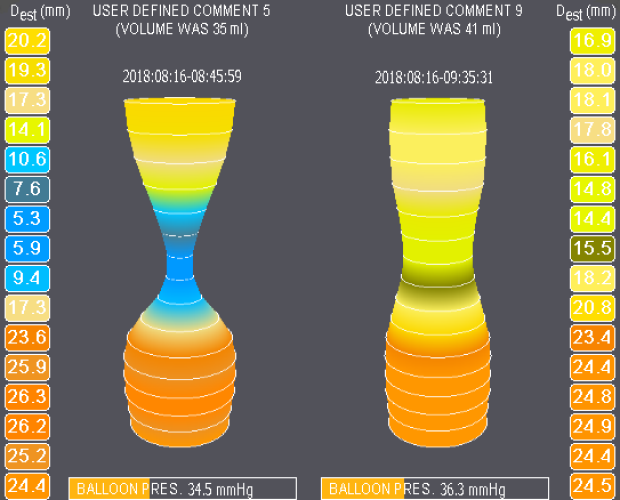
Patients suffering from upper GI disorders including gastroesophageal reflux, achalasia and pyloric stenosis have abnormal intestinal physiology. There is limited data on how the physiology of the GI tract is altered after surgical intervention.
The purpose of this investigation is to measure the diameter, compliance and distensibility of the intestine pre- and post-operatively in upper GI disorders and correlate these measurements with health outcome measures. The investigators hope to more precisely characterize the physiology of upper GI tract and correlate it to outcomes. This knowledge could help surgeons to better tailor interventions to a specific patient's physiology. Several studies have shown the use of an endoluminal functional lumen-imaging probe (FLIP; EndoFLIP®, Crospon Ltd, Galway, Ireland) in adults. These studies show the measurable difference in esophageal physiologic measure including diameter, compliance and distensibility. Further, investigators have used the EndoFLIP as an intraoperative tool. These researchers showed that using this tool they are able to better assess the success of the procedure in real time. In the current study conducted by Dr. Wall's research group, our researchers hope to evaluate differences in already approved standards of care and to identify long-term outcomes of pediatric patients according to their pre- and post-operative esophageal physiology.
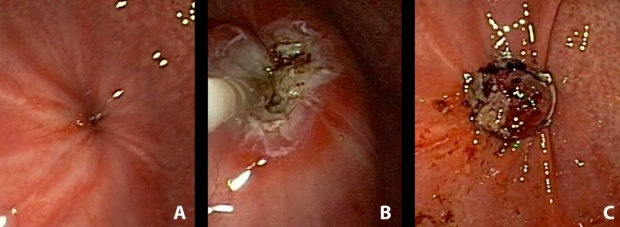
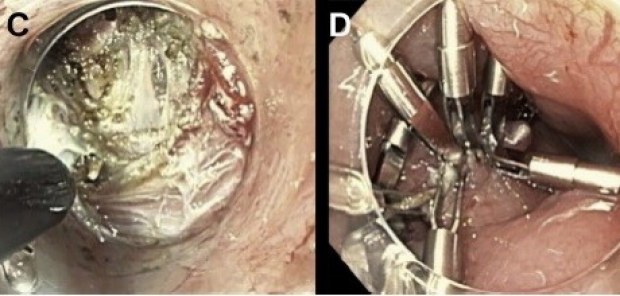
(A) Endoscopic View of GCF, (B) Endoscopic cauterization of the fistula, (C) Over the scope endoscopic clip sealing the GCF
Endoscopic Gastrocutaneous Fistula Closure
Gastrocutaneous fistula (GCF) occurs commonly in pediatric patients after removal of long-term gastrostomy tubes.
Although open repair is generally successful, endoscopic approaches may offer benefits in terms of incisional complications, postoperative pain, and procedure time. In addition, endoscopic approaches may offer particular benefit in patients with varied degrees of skin irritation or erosion surrounding a GCF, making surgical repair difficult, or patients with significant comorbidities, making minimal intervention and anesthesia time preferable. Over-the-scope (OSC) clips are a new technology that enables endoscopic closure of intestinal fistulas up to 2 cm in diameter. Dr James Wall’s research has found that Endoscopic GCF closure using an OSC clip is technically feasible in the pediatric population with good long term success in the first 20 cases.

Virtual Reality
Virtual Reality as a Tool for Biomedical Engineers to Identify Unmet Clinical Needs: the Use of VR for Clinical Observation
The identification of unmet clinical needs through direct clinical observations is central to the Stanford Biodesign approach to need-driven health technology innovation.
Unfortunately, access restrictions prevent the scalability of this approach when training undergraduate and graduate students from diverse backgrounds. Virtual Reality (VR) offers an alternative method for students to gain an immersive experience in clinical environments such as the operating room. The wall lab and the biodesign department is conducting several studies to compare VR to live observations for students seeking unmet clinical needs.
Myoelectric Activity of the Gut
Measurement of Gastrointestinal Myoelectric Activity in Pediatric Patients at Risk for or Who Have a Post-Operative Ileus (POI) After Major Abdominal Surgery
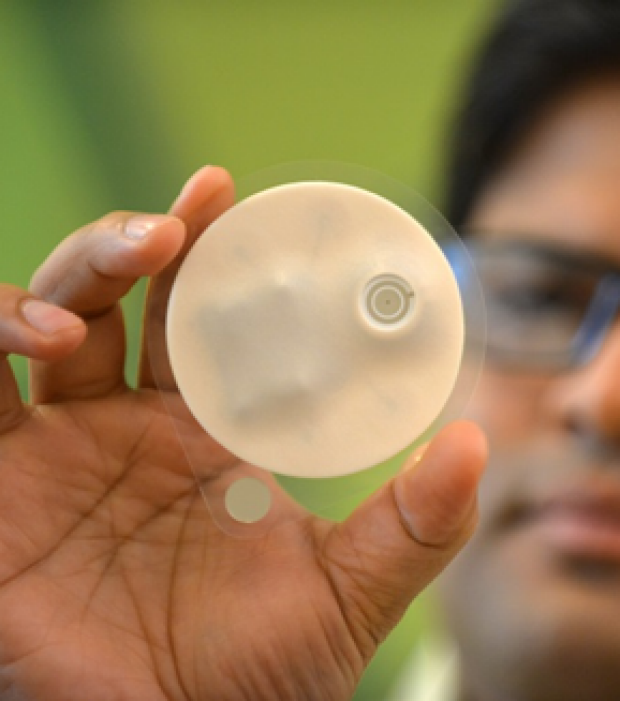
The disposable wireless patch (G-Tech Medical, Fogarty Institute for Innovation, Mountain View, CA) acquires myoelectrical signals noninvasively from the abdominal gastrointestinal tract within two hours of surgery.
The G-Tech wearable patch consists of a flexible substrate material approximately 2.7” diameter which are made up of Ag/AgCl electrodes, a medical grade adhesive, and electronics to acquire, digitize, and transmit myoelectrical data via Bluetooth Low Energy (BLE) to a paired iPod Touch App. The custom app has a patient interface to enter clinical information such as overall mobility, diet status, pain control, nausea or emesis, and the return of bowel function.
Postoperative ileus (POI) refers to obstipation and intolerance of oral intake due to factors that disrupt the normal coordinated propulsive motor activity of the gastrointestinal tract. Some degree of POI is a normal obligatory and physiologic response to abdominal surgery. The physiologic POI that typically follows surgery has a benign and self-limited course. Prolonged ileus results in longer hospitalization and warrants further work-up as a sign of peri-operative complications such infection or leak. A wide variety of endpoints have been used to measure gut recovery with no consensus as to which one is most clinically meaningful. Currently, return of GI function to normal is determined based on the passage of flatus or stool and tolerance of an oral diet within 4 days after surgery. Pathologic postoperative ileus is diagnosed on postoperative day 4 or after based on the following, mainly subjective, signs and symptoms: nausea or vomiting, inability to tolerate an oral diet over the preceding 24 hours, absence of flatus over the preceding 24 hours, and abdominal distention. Increasingly, post-operative protocols initial early feeding in low risk cases. However, time based feeding risks feeding a subset of prolonged ileus patients too early. No objective test exists to determine the ideal timing of post-operative feeding.
Objectively diagnosing and differentiating between physiologic and pathologic POI remains challenging as it largely depends on the patient's ability to sense and communicate signs and symptoms of POI and change of their GI function. This is particularly challenging in the younger pediatric population, as they that don't possess the skills and ability of speech and language. Therefore, there is a need to objectively assess and record gastrointestinal activity in pediatric patients who undergo major abdominal surgery for early detection and distinction between physiologic and pathologic POI. Previous studies have shown that myoelectric gastrointestinal activity can exhibit changes in patients who develop a postoperative ileus. Therefore, a promising technology to diagnose and help differentiate between a pathological POI and physiological POI could potentially be found in measuring myoelectric gastrointestinal and colonic activity with the Gut Check disposable wireless patch from G-Tech Medical (G-Tech Medical, Fogarty Institute for Innovation, Mountain View, CA).
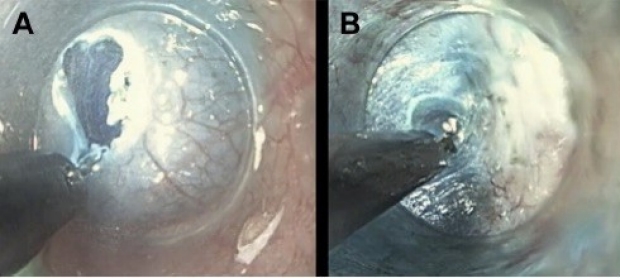
(A) Mucosal incision, (B) Dissection of the submucosal plane exposing circular muscle fibers, (C) Selective division of circular muscle fibers with preservation of underlying longitudinal muscle fibers, (D) Closure of mucosal incision with endoscopic clips
POEM
Per-Oral Endoscopic Myotomy
Achalasia is a primary esophageal motility disorder characterized by aperistalsis of the esophagus and failed relaxation of the lower esophageal sphincter that presents rarely in childhood.
The peroral endoscopic myotomy (POEM) procedure is an emerging treatment for achalasia in adults that has recently been introduced into pediatric surgical practice. The Wall group conducted a prospective cohort study of all children referred to Stanford University Lucile Packard Children's Hospital with manometry-confirmed achalasia who underwent a POEM procedure from 2014 to 2016. The study enrolled 15 subjects ranging in age from 7-17 years and showed that the POEM procedure can be successfully completed in children for the treatment of achalasia with demonstrated short-term post-operative improvement in symptoms. The POEM procedure is showing promise with similar function outcomes to surgery with less post-operative discomfort.
Translational Projects
Stanford Pediatric Device Consortium Supports COVID Care Innovation
As COVID-19 cases started to escalate in the US, Stanford's Pediatric Device Consortium (PDC) supported innovators working to rapidly address needs created or exacerbated by the pandemic. Seed funding was granted to three Stanford-affiliated projects, ensuring that pediatric care was incorporated from early design through implementation of the projects.
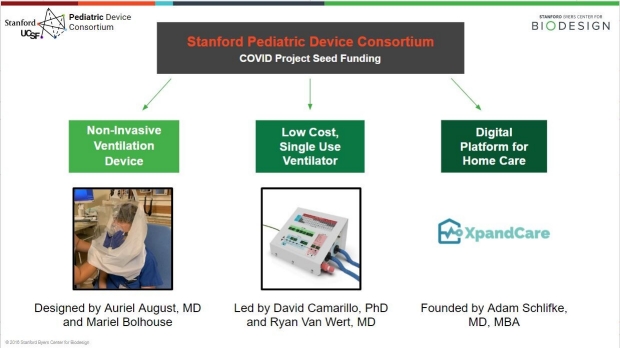
Re-Enabling Positive Pressure Ventilation
Auriel August, MD and Mariel Bolhouse engaged in two weeks of COVID-related needs finding as part of the Stanford Biodesign Innovation Fellowship. They found that COVID patients were often intubated without first attempting non-invasive respiratory support measures, such as positive pressure ventilation (PPV). This was due to the hazardous respiratory aerosols that accompany CPAP and BiPAP device use. Six weeks later, August and Bolhouse are on their fourth prototype of a novel adjunctive device designed to contain aerosols and safely re-enable PPV use.
Funding from the PDC will support initial manufacturing of the device, which the team has committed to developing for all ages. The device has gone through multiple rounds of usability and efficacy testing, aiming to fit into the current infrastructure for PPV use and ensure safety measures equivalent to the use of an N-95 mask. While the team is currently striving to build an evidence base beyond what is required by the FDA Emergency Use Authorization (EUA) Pathway, they recognize the external pressure to manufacture their product before a potential second wave of COVID cases.
As the team finalizes their design, they have submitted testing plans to the FDA and are actively working to determine the right contract manufacturing partner. After testing is complete by the end of June, the team hopes to see uptake of the product across the US and Europe, where PPV typically serves as an important step of respiratory support for patients that fail nasal cannula. In the long-term, the team hopes the product can join PPV company portfolios that have the capability to efficiently distribute the adjunctive device.

Low Cost, Single-Use Ventilation for All Ages
As the threat of a national ventilator shortage became apparent, David Camarillo, PhD felt that his Stanford lab’s work with electromechanical devices made his group well suited to contribute to a solution. After a Friday night group huddle in mid-March, Camarillo and Sam Raymond, PhD launched their work on new ventilation designs and testing with the help of the engineering firm 219 Design. The team, now co-led by Camarillo and Ryan Van Wert, MD, has since developed a low-cost precision ventilator that can be used for neonates through adults.
A Stanford PDC grant was the first investment to catalyze building the new ventilator. The team has since raised nearly $1M and submitted an FDA application. They have been supported by lead clinical advisors David Cornfield, MD and Brett Ley, MD, as well as by the Chan Zuckerberg Biohub. The technology uses hospital wall gas O2 and a precision valve which allows for delivery of small volumes of air, appropriate for neonates. Most of the rapid low-cost COVID-19 ventilators built by other universities include an AMBU bag squeezing mechanism which is not sufficiently precise for the small volumes required for neonates.
Six months after starting the project, the team submitted an Emergency Use Authorization to the FDA for the ventilator. Although the current indication is for COVID-19 in the USA, this low cost technology may prove even more useful for neonates and young children in developing nations where they cannot afford a high-cost precision ventilator. The team is therefore exploring international partnerships to allow for local manufacturing and distribution of the product in countries hit hardest by ventilator shortages, including Brazil, India, and Mexico. The group is also considering following the model of NASA’s Jet Propulsion Laboratory, which received FDA approval for their ventilator design and solicited proposals for international licensees.

Digital Platform for Home Care
In March 2020, anesthesiologist Adam Schlifke, MD, MBA wrote a call to action and operational plan for COVID critical care that included a shift in patient care settings. With a shortage of hospital beds and overburdened providers, Schlifke believed that patients should avoid hospitals until critical care services are needed for an extended period. This idea has since developed into the company XpandCare, a new platform to allow for the integration of digital health tools for patient home care and monitoring.
As a seasoned entrepreneur, Schlifke recognized the challenges of raising funding during COVID, but was able to work through the legal and administrative costs of establishing the company with initial seed funding from the PDC. The receipt of PDC funding ensured that the platform was designed from the start with pediatric patients in mind.
XpandCare is a vendor agnostic platform that works across three layers of the digital health ecosystem to support the care of COVID patients. The front-end consists of partnerships with innovative digital technology companies for connected pulse oximeters, thermometers, ultrasounds, and EKGs. These devices allow patients to remain home while data is collected and reported back to healthcare providers. Providers can then respond to patient data and needs through the ecosystem’s middle-layer, telehealth. XpandCare has partnered with Bluestream Health, a web-based software that empowers, rather than employs, physicians through simple software and the availability of on-demand translators for 200 languages. The back-end handling of the healthcare data itself is built by XpandCare.
Schlifke believes this redesigned healthcare system allows for improved resource allocation and removes the financial incentives that accompany large hospital systems. Through continued growth and partnerships, XpandCare aims to build a future where increased bed capacity and spending is replaced with broader adoption of high-tech, low-cost tools.

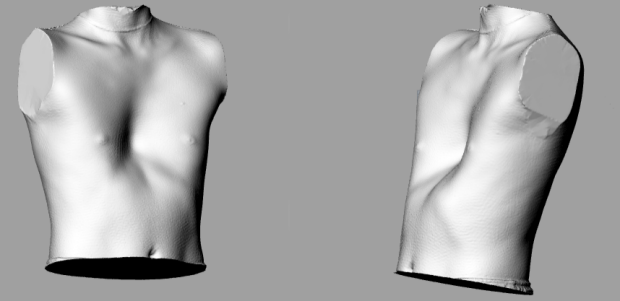
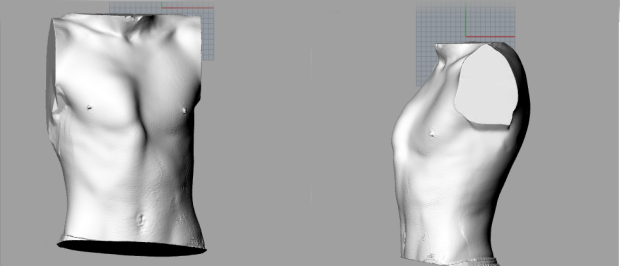
Chest Wall Deformities
From optical imaging to Finite Element Analysis: to create a model for rapidly testing smart and dynamic braces interventions and iterations
Pectus Excavatum
Pectus Carinatum
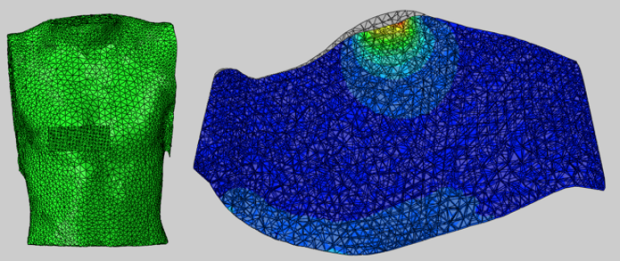
Finite Element Analysis
Pectus excavatum (“sunken chest”) and pectus carinatum (“pigeon chest”) are the two most commonly observed chest wall deformities. Pectus excavatum is characterized by the depression of the sternum and costal cartilages, while pectus carinatum involves the sternum being displaced outward.
The most widely accepted metric to assess the severity of either condition is the Haller index, and was created by Haller et al. in 1987. The Haller index is defined as the transverse distance from rib to rib divided by the anterior-posterior distance from sternum to spine. These measurements have been traditionally taken from a computed tomography (CT) scan, but recent studies have shown that lateral and anterior-posterior chest x-rays can provide the same information with much less exposure to radiation required. The Wall group is investigating the accuracy of using new optical imaging technology to map the contour of the chest wall in patients with chest wall deformities. The advent of 3D optical scanners presents an opportunity to image patients without any radiation. The aims of the current study is to use cross-sections of the chest from 3D scans to obtain measurements for a modified Haller index, and compare precision both within individual raters and between different raters. Preliminary results of this study evaluating the reproducibility of measurements taken from these 3D scans, shows promise and suggests that this technology may provide a viable alternative to the current standard of using CT scans or x-rays to document these conditions. The use of this new technique also presents an opportunity for patient progress to be tracked closely while in treatment, given the ease of scanning and the lack of radiation involved. Finally, 3D scans that can be measured reliably will allow for more accuracy when designing custom-fit braces and other devices for patient use.
Posterior Urethral Valve Obstruction
Posterior urethral valves (PUV), a type of lower urinary tract obstruction, is a congenital condition where excess tissue obstructs the posterior urethra. PUV has an incidence of 2.2 in 10,000 births, or nearly 900 cases annually in the United States. It only occurs in boys and may have a genetic component. In patients with PUV, the blockage of flow causes a buildup of urine in the bladder and vesicoureteral reflux (reverse flow). Up to 30% of children born with PUV progress to end-stage renal disease by adolescence, requiring dialysis and kidney transplant for survival. PUV patients also suffer from bladder and lung dysfunction, and they require extensive lifelong care.
The current treatment, a vesicoamniotic shunt, is effective at restoring fluid but has a risk of dislodgement. If dislodgement occurs, the patient requires an additional surgery to insert a replacement shunt, and each repeat surgery is life- threatening. This risk is largely due to the incision into the amniotic sac which can rupture the membrane, inducing dangerously premature labor. The larger the incision, the greater the risk.
Dr James Wall’s research team is currently working on the development of a novel way of restoring amniotic fluid with minimum risk to the fetus and the mother.
Graduated Projects
Novonate

Novonate was developed within the premises of the Biodesign Program and under the mentorship of Dr James Wall. Umbilical catheterization is a lifeline for delivering medication and nutrition to critically ill newborns in the neonatal intensive care unit. The rate of bloodstream infections attributed to umbilical catheters is at least five times greater than that of adult central lines. Proposed causes of this elevated infection rate include migration of bacteria after insertion, caretaker contact of catheter-stump interface, and movement of the catheter after insertion. The current standard of care for securing umbilical catheters consists only of a suture and non-sterile tape, which leads to variable securement and does not at all protect the catheter insertion site. Novonate standardizes and simplifies the process of umbilical catheter securement, enhances protection of the umbilical stump, and minimizes potential catheter translation. The product is designed to reduce infection risk by protecting the catheter insertion site from bacteria and stabilizing the umbilical catheters. LifeBubble is currently in pilot trials in US Neonatal Intensive Care Units.
In the News
IT TAKES A UNIVERSITY: HOW A DETERMINED TEAM DEVELOPED A TECHNOLOGY TO PROTECT VULNERABLE NEWBORNS
“Although only about 200,000 newborns need umbilical catheters every year [in the US], one in five acquires a costly and dangerous bloodstream infection,” said team member Eric Chehab, who was a graduate bioengineering student at the time. And this is despite the fact that the nurses watch over these babies really carefully because they are so vulnerable.”
Solving a big problem, among some of the littlest patients
“It took more than five years and the efforts of a lot of dedicated people to make this solution viable,” said Wall. “It is an incredibly important unmet need—literally saving premature babies. By utilizing a full range of university resources, including students, facilities and internal grants, we were able to develop the device to the point that it could attract funding—which would never have happened using traditional methods—and it is now on a path to reaching patients within the next year.”
Select Publications
Initial Experience of Peroral Endoscopic Myotomy for Treatment of Achalasia in Children. Kethman W. Thorson C, Sinclaire T, Berquist W, Chao S, Wall J. J Pediatric Surg. 2017 Epub ahead of print
Trends and Surgical Outcomes of Laparoscopic vs. Open Pyloromyotomy in the United States. Kethman WC, Harris AHS., Hawn MT, Wall J. Surg Endosc Surg Endosc. 2018 Jan 16
Dilation of Esophageal Stricture in a Pediatric Patient Using Functional Lumen Imaging Probe Technology Without the Use of Fluoroscopy. Taylor JS, Danzer E, Berquist WE, Wall J. J Pediatr Gastroenterol Nutr. 2018 Aug;67(2):e20-e21
An in vitro bacterial surface migration assay underneath sterile barrier material commonly found in a hospital setting. Shih JD, Wood L Dambkowski CL, Torres S, Chehab E, Venook R, Wall J. J of Perinatology. Epub ahead of print Mar. 2017
Endoscopic Division of Duodenal Web Causing Near Obstruction in 2-Year-Old with Trisomy 21. Wood LS, Kastenberg Z, Sinclair T, Chao S, Wall JK. J Laparoendosc Adv Surg Tech A. 2016 May; 26(5):413-7
Endoscopic Submucosal Dissection of a Large Hamartoma in a Young Child.Wall J, Esquivel M, Bruzoni M, Wright R, Berquist W, Albanese C. J Pediatr Gastroenterol Nutr. 2016 Jan; 62(1):e5-7
In-vitro assessment of bacterial colonization rates of goat umbilical cord segments using three embodiments of a novel neonatal umbilical catheter protection device. Dambkowski C, Chehab E, Shih J, Venook R, Wall J. BMJ Innov 2016 Mar; 2:2 93-98
Salvage of a failed open gastrocutaneous fistula repair with an endoscopic over-the-scope clip.Jamirillo J, Wall J. J Pediatr Surg Case Reports. Published Online Mar. 2016
Introduction of the Per-Oral Endoscopic Myotomy technique to pediatric surgical practice.Chao S, Rivas H, Wright R, Russo M, Wall J. J Pediatr Surg Case Rep 2014 June; 2(6) 313-315.
Intraoperative functional luminal imaging to assess esophagogastric junction distensibility during Per-Oral Endoscopic Myotomy in pediatric patients. Wright R, Chao S, Wall J. J Gastroint Dig Syst 2014 Aug; 4:207
Initial results of endoscopic gastrocutaneous fistula closure in children using an over the scope clip.Wright R, Abrajano C, Koppolu, R, Stevens M, Nyznyck S, Chao S, Bruzoni M, Wall J, J Lap Advanced Surg Techniques 2015 Jan; 25(1):69-72.
MAGNAMOSIS IV: magnet compression anastomosis for minimally invasive colorectal surgery. Wall J, Diana M, Leroy J, DeRuijter V, Gonzales KD, Lindner V, Harrison M, Marescaux J. Endoscopy. 2013 Aug; 45(8):643-8.
Submucosal Endoscopic Myotomies for Esophageal Lengthening: A Novel Minimally Invasive Technique with Feasibility Study. Wall J, Perretta S, Diana M, Dhumane P, Alvar Haro JI, Dallemagne B, Becmeur F, Krummel T, Marescaux J. Eur J Pediatr Surg. 2012 Jun;22(3):217-21
The Impact of Postgraduate Health Technology Innovation Training: Outcomes of the Stanford Biodesign Fellowship. Wall J, Hellman E, Denend L, Rait D, Venook R, Lucian L, Azagury D, Yock PG, Brinton TJ. Ann Biomed Eng. 2017 May;45(5):1163-1171
Research Team Alumni

Vivian Emmely de Ruijter
Current Role: Senior Manager at Manatt Healthcare Consulting in Digital and Technology
Vivian’s health technology innovation journey started early during her medical studies. More Despite the satisfaction she found in practicing medicine, she’s always been interested in how to improve it.Because Vivian believes that this will require improvements in not only in medicine, but also technology and design, she has dedicated her career to advance innovation in healthcare. She completed several fellowship programs in surgical innovation in parallel and after her medical school in the Netherlands, among others at the IRCAD, a world renowned center in minimally invasive surgery in France; at the Stanford General Surgery department, and a Biodesign Innovation Fellowship at the Stanford Byers Center for Biodesign. These programs taught her how to identify important unmet healthcare needs through clinical observations, developing innovative diagnostics, therapeutics, devices and digital technologies to address them. Although Vivian has learned much in these endeavors, she knows that she still has much to learn become a successful aspiring life sciences innovator and investigator for applications in the pediatric population, which she thrives to acquire through her fellowship at the pediatric surgery department.